Injecting insulin correctly is an important part of your patient’s diabetes management1
Proper injection technique can help lower A1C2*
In a study of patients with diabetes who inject insulin, patients educated on proper injection technique (including using a new needle for every injection, rotating injection sites, and shifting to a 4mm or 5mm needle) experienced a 1% reduction in A1C at 6 months.2*

Components of proper injection technique training include
Using a new needle
Rotating injection sites
Using a shorter needle
Remind your patients to use a new needle every time they inject
Using a new needle matters because:
- Nearly 50% of patients with diabetes reuse their needles.3†
- Reuse has been associated with increased risk of developing lipohypertrophy,1,4 which can contribute to erratic insulin absorption, increased glycemic variability, and unexplained hypoglycemic episodes.1,4‡
- Patients who were provided an adequate supply of needles and proper injection training reported no reuse of needles.2*
Encourage your patients to rotate injection sites
Lipohypertrophy, or lipo, can be caused by incorrect injection site rotation. Injection site rotation appears to be the most important factor in protecting against lipo.5
Download Tummy Template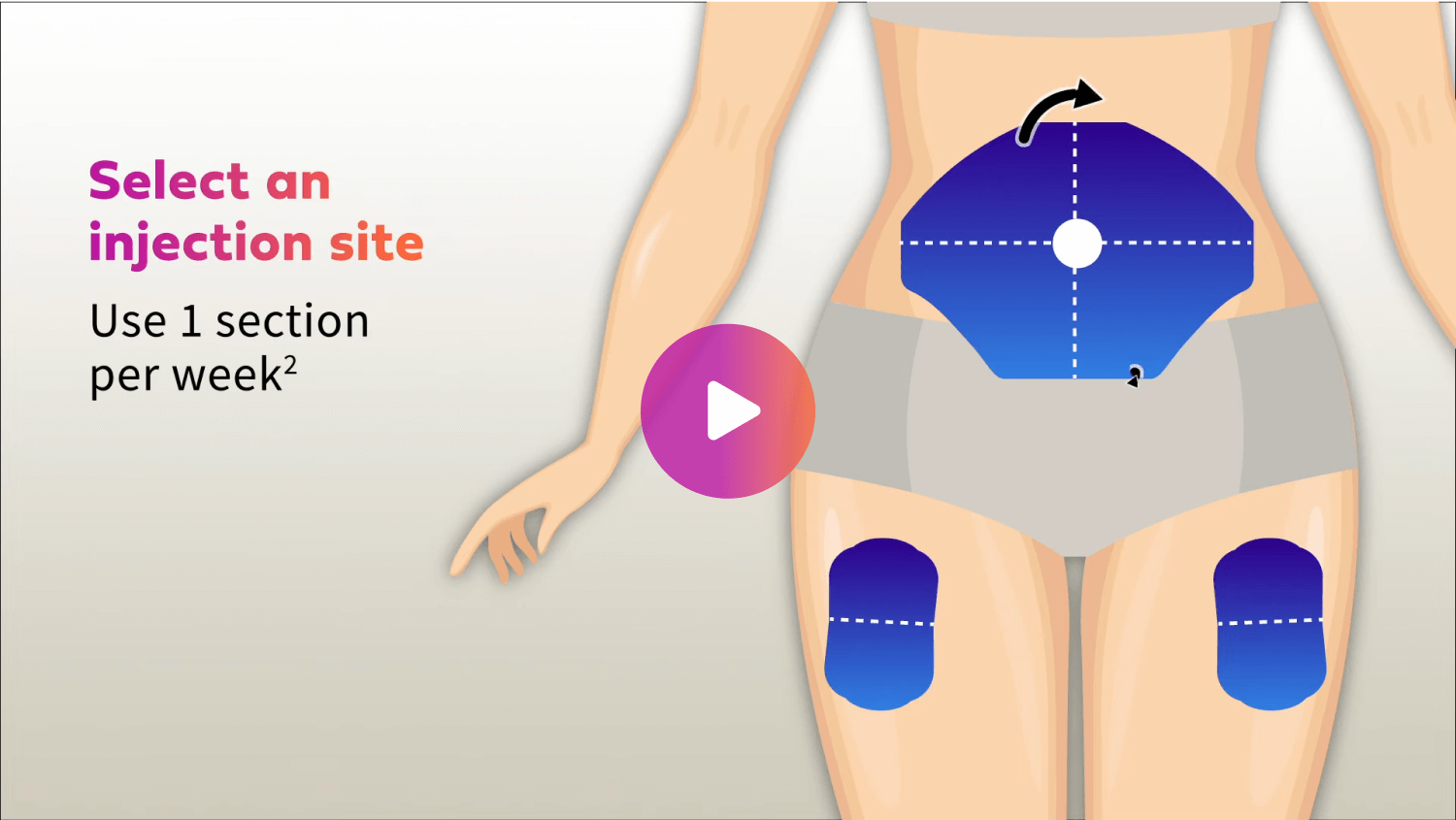
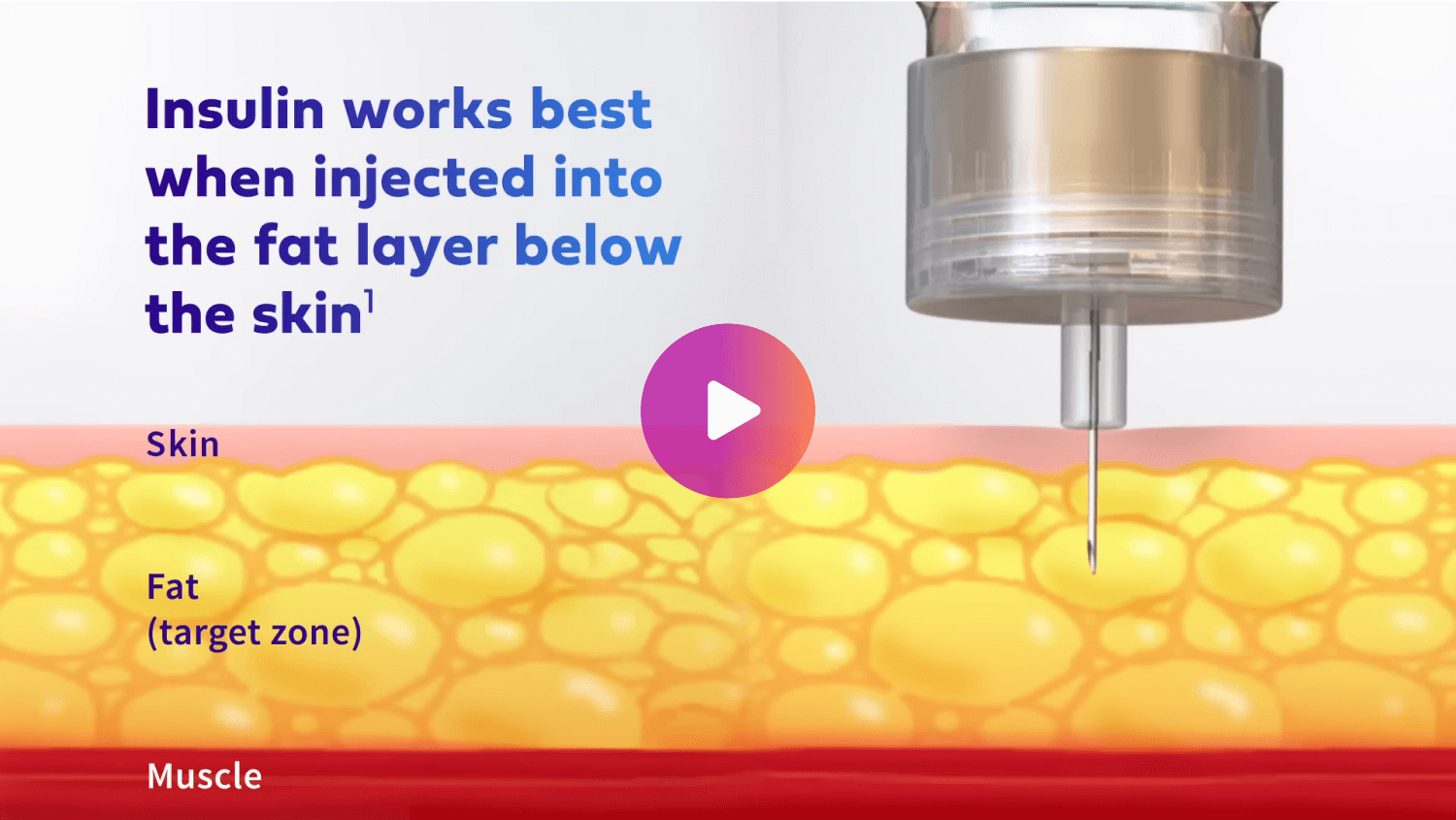
Consider prescribing shorter needles for your patients
Longer needles can increase the chance of injecting into the muscle. Clinical recommendations state that a 4mm pen needle or 6mm insulin syringe is the recommended needle length for all patients.1
Resources to share with patients who are new to insulin therapy


See how Micro-Fine UltraTM Pen Needles can help improve the injection experience
Learn Moreembecta, formerly part of BD, is now one of the largest pure-play diabetes management companies in the world. This singular focus allows us to leverage our 100-year legacy in insulin delivery, while empowering people with diabetes to live their best lives.
Learn About Us*116 patients with diabetes on insulin were randomized to 3 intervention groups to assess the change from baseline in A1C at 6 months following structured injection technique training and changing to a shorter needle length (4mm or 5mm pen needle). Baseline A1C for all groups was similar (mean: 8.5-8.8% [± 1.4-1.9%]).
†13,289 patients with diabetes who inject insulin participated in an ITQ survey. 38.8% of the 2,711 patients using insulin syringes reported needle reuse. 55.8% of the 11,961 patients using pen needles reported needle reuse.
‡A casual relationship has not been established. 13,289 insulin-injecting patients participated in a survey. Needle resuse was assessed through a questionnaire and lipohypertrophy (LH) was assessed through a questionnaire and HCP assessment using visual and palpation methods. Logistic regression analysis was used to find the association between pen needle reuse and LH (P=0.2).
References
1. Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations. Mayo Clin Proc. 2016;91(9):1231-1255.
2. Misnikova IV, Gubkina VA, Lakeeva TS, Dreval AV. A randomized controlled trial to assess the impact of proper insulin injection technique training on glycemic control. Diabetes Ther. 2017;8(6):1309-1318.
3. Frid AH, Hirsch LJ, Menchior AR, Morel DR, Strauss KW. Worldwide injection technique questionnaire study: population parameters and injection practices. Mayo Clin Proc. 2016;91(9):1212-1223.
4. Frid AH, Hirsch LJ, Menchior AR, et al. Worldwide injection technique questionnaire study: injecting complications and the role of the professional. Mayo Clin Proc. 2016;91(9):1224-1230.
5. Blanco M, Hernández MT, Strauss KW, Amaya M. Prevalence and risk factors of lipohypertrophy in insulin-injecting patients with diabetes. Diabetes Metab. 2013;39(5):445-453.
These devices are UKCA-marked in accordance with UK Medical Device Regulations.